

CORONAVIRUS: FREQUENTLY ASKED QUESTIONS FROM CANCER PATIENTS
How can I protect myself from infection? “As with the flu and other acute respiratory illnesses, the most important protective measures are compliance with […]
How can I protect myself from infection? “As with the flu and other acute respiratory illnesses, the most important protective measures are compliance with […]

Explaining cancer to children is a major challenge for adults. But it is important to talk to children about cancer. In this article we will provide you […]

With nanotechnology, gold and lasers: At the University of Duisburg-Essen, researchers are developing an unusual method to stop the growth of tumors. NANOTECHNOLOGY: SCIENCE OF […]
Britta Bürgers had just become a mother when she lost her husband to cancer. Nine years later, she was also found to have a tumor. Here she […]

Some types of cancer are caused by the human papillomavirus – HPV for short. An effective vaccination against HPV is available. It lowers the risk of mouth, […]

Would you like to donate your hair and do something good with it? In the following article we answer frequently asked questions about donating hair. A note […]

CHILDREN IN THE FOCUS OF THE GERMAN CANCER AID When Mildred Scheel founded the German Cancer Aid in 1974, her focus was not only on […]
Should I consider taking vitamins and nutritional supplements before, during, or after chemotherapy?Consult your doctor, nurse or dietitian about the use of nutritional supplements such […]
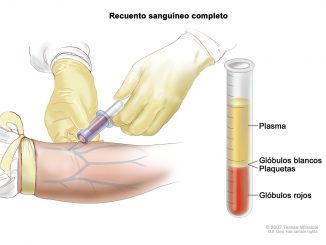
When a person presents symptoms such as weakness, loss of appetite and weight loss associated with repeated infections or bleeding problems, especially if these appear […]

THIS IS HOW TOBACCO INCREASES YOUR RISK OF CANCER (AND NOT JUST LUNG CANCER) Tobacco continues to be one of the biggest public health problems. According […]
Copyright © 2025 | WordPress Theme by MH Themes